












If you are thinking about how to add FUE to your practice, the marketing is the easy part. Most practice owners underestimate the operational lift. Credentialing, room setup, equipment, staffing, consumables, compliance, and patient flow all need to be solved before the first case books. This checklist walks through what it takes to launch follicular unit excision profitably.
FUE is one of the fastest growing aesthetic procedures in the world. ISHRS practice census data has shown FUE adoption climbing every year since 2014, and it now represents the dominant surgical hair restoration technique among member surgeons.
Why add FUE to your practice now
The case for adding FUE in 2026 is the combination of mature demand and a mature device market. Aesthetic and dermatology practices want service lines that combine cash pay revenue, strong margins, and predictable demand. FUE checks all three. Cases run $4,000 to $15,000 depending on graft count, the procedure does not depend on insurance reimbursement, and patient demand keeps trending up across male and female demographics.
What makes 2026 different is that the device market has matured. Manual punch systems, motorized handpieces, and robotic platforms each have established workflows and training pathways. The decision now is which device path fits the practice model, the surgeon’s skill profile, and projected case volume.
Clinical credentialing and training
The clinical credentialing path is the first decision, before any equipment purchase, marketing plan, or operatory build. Most state medical boards allow physicians with surgical training to perform FUE, but each state has its own rules on technician supervision, scope of practice for non-physician operators, and informed consent. Verify with your state board in writing.
For surgeons new to hair restoration, the credible training pathway runs through the International Society of Hair Restoration Surgery. The ISHRS publishes FUE clinical practice guidelines and educational resources, runs the annual world congress, and maintains content that practicing physicians use to build competency. Plan on 6 to 12 months of structured training, observation, and proctored cases before scheduling independent procedures.
Technician training and team build
FUE is a team procedure. A typical case runs 4 to 8 hours and requires at least 2 trained technicians working alongside the physician. Building this team is often the longest lead time item when you add FUE to your practice. Options include hiring experienced technicians from the hair restoration industry, partnering with a traveling technician group on a per-case basis, or training your own staff through formal programs.
The operatory setup when you add FUE to your practice
FUE does not require a full surgical suite, but the room you use needs to meet specific clinical and regulatory standards. Plan for a dedicated procedure room of at least 200 square feet with the patient chair as the centerpiece and clear circulation space on three sides for the surgical team.
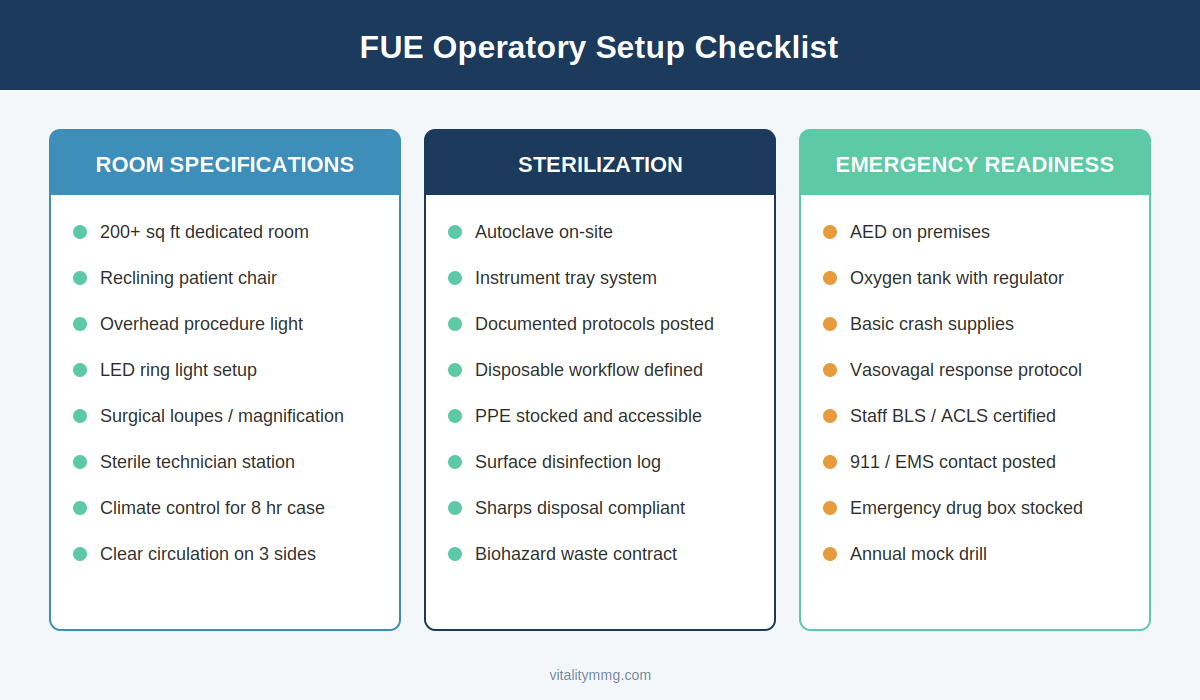
Three non-negotiable categories for any room running FUE cases: room specifications, sterilization protocols, and emergency readiness.
Lighting matters more than most practice owners expect. Surgical loupes plus an overhead procedure light or LED ring light setup is the baseline. Magnification is non-negotiable for graft extraction quality. Add a comfortable reclining patient chair rated for long procedures, a sterile workstation for the technician team, and adequate climate control to keep the patient and the staff comfortable through an 8 hour case.
Sterilization and emergency readiness
Sterilization protocols need to be documented and posted in the room. Autoclave, instrument tray system, and disposable workflow all need to be defined before the first case. Emergency readiness includes an AED, oxygen, basic crash supplies, and documented protocols for vasovagal response, which is the most common adverse event during long procedures under local anesthesia.
Equipment and device selection
The capital equipment decision is the largest single financial commitment when you add FUE to your practice. Three device tiers exist, and each has a different economic and operational profile.
Manual punch systems are the lowest entry cost, typically under $5,000 for a complete set, but they place the entire graft extraction burden on the surgeon’s hand technique. Motorized handpieces in the $15,000 to $40,000 range speed up extraction and reduce surgeon fatigue. Robotic platforms like ARTAS sit in the $200,000 plus range with ongoing per-case consumable costs, but they offer reproducible extraction, marketing differentiation, and the ability to delegate parts of the workflow.
Your case volume projection drives the right answer. Practices forecasting under 50 cases per year almost always start with manual or motorized handpieces. Practices targeting 100 plus cases annually often justify the robotic investment through speed, consistency, and marketing leverage. Our team works with practices on the marketing side of ARTAS robotic lead generation and can model the economics either way.
Consumables and initial supply stocking
The capital decision gets the attention; the consumables decision gets overlooked. A first-year practice running 30 to 50 cases will spend more on consumables than most owners budget for.
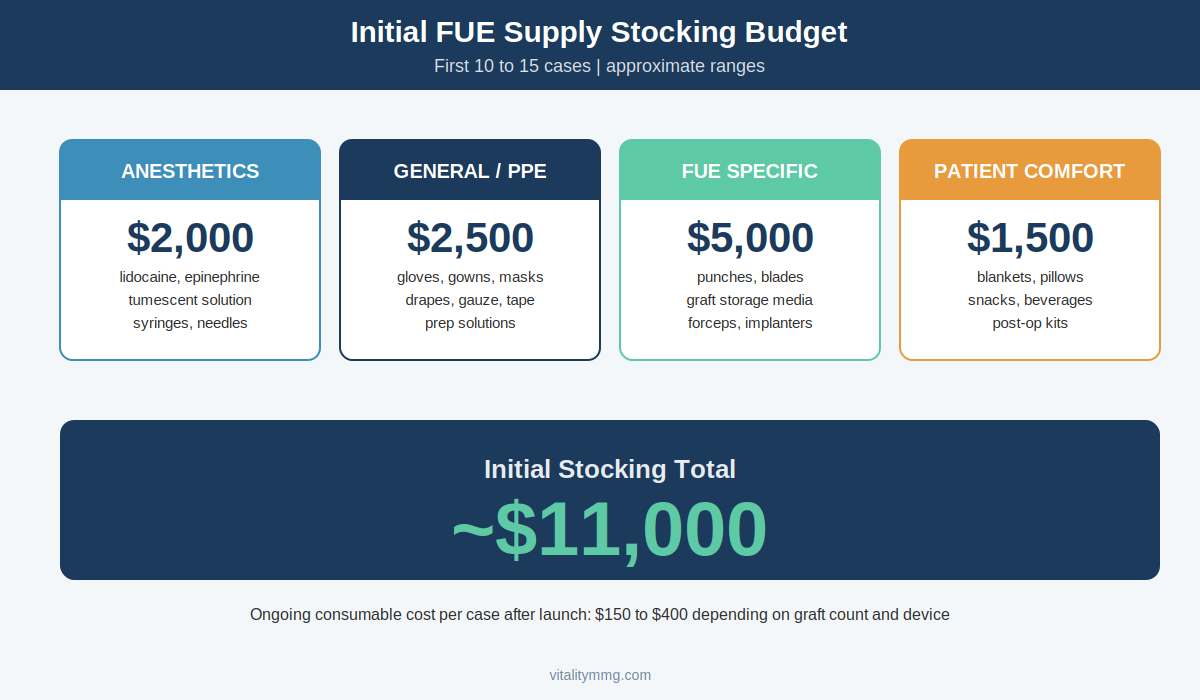
Initial stocking budget for the first 10 to 15 cases totals roughly $11,000 across four categories. Ongoing per-case cost runs $150 to $400.
Initial stocking falls into four categories: anesthetics and injection supplies, general surgical and PPE supplies, FUE-specific items like punches and storage media, and patient comfort items. Plan on roughly $11,000 to fully stock the procedure room for the first 10 to 15 cases. After that, ongoing consumable cost per case typically runs $150 to $400 depending on graft count and device choice.
Build a vendor relationship with a hair restoration supply specialist rather than piecemealing the order through general medical distributors. The specialists carry the punches, storage media, and instruments that general suppliers do not stock.
Marketing and compliance for the new service line
Once the operational side is solved, the marketing side determines whether the room stays full. FUE marketing is more regulated than most aesthetic services because hair loss intersects with FDA drug claims, FTC advertising rules, and platform-specific medical advertising restrictions on Google and Meta.
Build the marketing foundation correctly the first time. That means a service page that meets hair transplant marketing compliance standards, before and after content with proper consent documentation, and ad creative that avoids the negative self-perception language that triggers Meta disapprovals. Skipping any of these creates account level risk that takes months to undo.
Lead generation channels
The channels that work for FUE are not the same channels that work for general aesthetics. Search intent for hair restoration is strong and high commercial value, which makes hair restoration lead generation through Google search the highest ROI starting point for most new practices. Paid social plays a supporting role for awareness and remarketing rather than direct response.
A realistic 6 month rollout
Practices that try to add FUE to their service line in 60 days almost always have a rough launch. Six months is realistic from decision to scaled case volume.
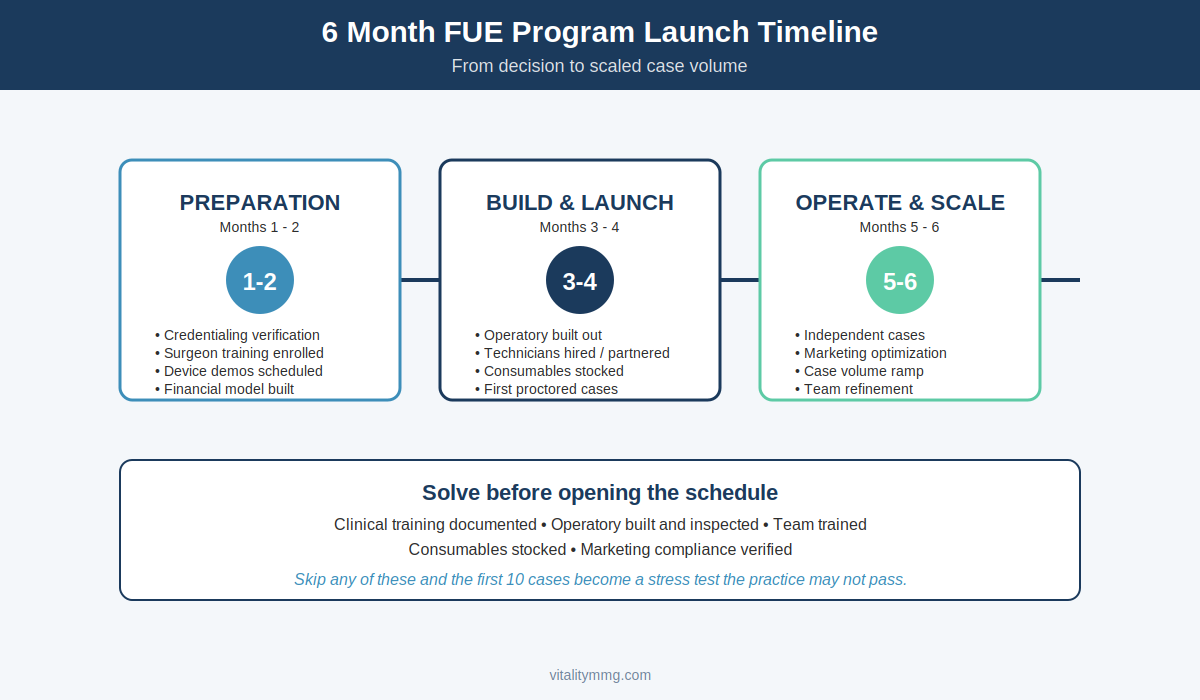
A realistic 6-month rollout from financial modeling through scaled case volume, broken into preparation, build and launch, and operate and scale phases.
Months 1 and 2 are preparation: credentialing verification, surgeon training enrollment, device demos, financial modeling, and operatory planning. Months 3 and 4 are build and launch: room buildout, technician hiring or partnership, consumable stocking, marketing foundation, and first proctored cases. Months 5 and 6 are operate and scale: independent cases, marketing optimization, case volume ramp, and team refinement.
What to solve before you open the schedule
The practices that succeed when they add FUE to their practice solve five things before they accept the first deposit. Clinical training completed and documented, operatory built and inspected, team hired and trained, consumables stocked, and marketing compliance verified. Skip any of these and the first 10 cases become a stress test that the practice may not pass.
Where VMMG fits
The clinical side is solvable with the right training partners and device vendors. The marketing side is where most practices either accelerate or stall. We work specifically with hair restoration practices on compliant lead generation, paid media, website conversion, and the operational marketing pieces that turn a new service line into a profitable one.
If you are planning to add FUE to your practice in the next six months, the marketing foundation should be built in parallel with the clinical buildout, not after. Call us at 631-919-0009 or book a consultation to map out the launch plan.